
http://s-media-cache-ak0.pinimg.com/736x/ca/7b/55/ca7b550006f1298cf639092177154c70.jpg
Posted by Waly Cardona – 7 Superfoods for Your Health #Superfoods #Weightloss
http://s-media-cache-ak0.pinimg.com/736x/ca/7b/55/ca7b550006f1298cf639092177154c70.jpg

http://s-media-cache-ak0.pinimg.com/564x/fc/b3/54/fcb354286c669e5687fbe935c9e3156d.jpg
Posted by Deana Whitaker – These eight spices will make any meal lively with an added bonus of faster metabolisms, fat fighting nutrients and more! #Weightloss #Spices

http://s-media-cache-ak0.pinimg.com/736x/65/64/df/6564df1f4922ecfe50ca05e9b3312857.jpg

https://s-media-cache-ak0.pinimg.com/564x/b6/ab/55/b6ab5514200ba959e35f8a0e5ce748dd.jpg
Posted by Veronica Joiner – Here is some information on the Symptoms of Celiac Disease
Unfortunately, many people who suffer from Celiac disease have no symptoms. This is particularly dangerous as intestinal damage can occur even when no symptoms are present. With new screening techniques, people are being diagnosed without ever suspecting they have the disease. It is important for people with no symptoms but a positive diagnosis to eat properly, as they are still at risk for serious complications of Celiac disease, such as cancer.
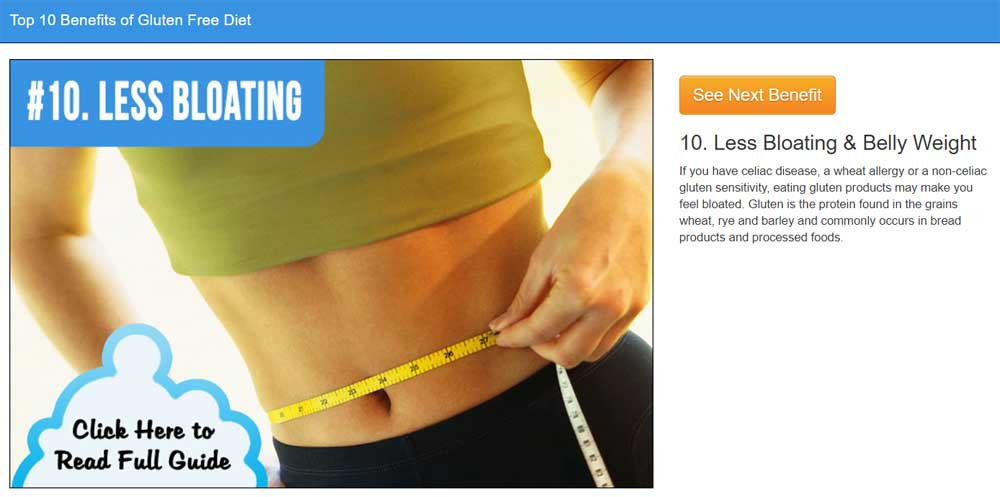
Many people who have Celiac disease suffer from painful bloating. For days after consuming gluten, the stomach may be distended and filled with gas. This can be quite painful. Many people complain of intestinal pain and the feeling of being “6 months pregnant”. They may also suffer from excessive gas and flatulence. Bloating can be symptoms of other dietary conditions, so look for it in conjunction with the consumption of gluten.
Chronic diarrhea is a common symptom of those afflicted with Celiac disease. The episodes may be smelly, explosive, and painful. The color of the stool may be pale or white, and typically floats on the surface of the water. Even solid stools may present these conditions. Related symptoms to chronic diarrhea include hemorrhoids. These can occur when there is not enough substance in the stools.
While diarrhea is common in Celiac sufferers, some people may be afflicted with constipation. This if from the body sluggishly moving the contents of the bowels. The body may be trying to pull all the nutrients possible from the food as the damaged villi will not work as efficiently. The constipation may be marked by periods of heavy diarrhea as the person consumes gluten. The constipation may cause pain and bloating.
Many people who suffer from Celiac disease lose weight as their body reacts to the missing nutrients. The diarrhea caused by gluten may stall the absorption of calories from the food, purging the body from its fuel. Conversely, a sufferer may in fact gain weight instead of lose it. Their bodies may be screaming for nutrients, so they eat in excess to achieve proper nutrition. They may have a hard time losing weight until they restrict gluten from their diet.
Fatigue is a common complaint of those affected by Celiac disease. Undiagnosed Celiac suffers may have their bodies suffer from malnutrition caused by absorption issues. Their body will respond with extreme fatigue and malaise in response. They may crave sugary foods and drink excessive caffeine just to stay energized. After diagnosis and the removal of gluten from the diet, fatigue may be the first symptom to be eliminated.
People who suffer from Celiac disease may experience something called a “brain fog” in relation to the consumption of gluten. This symptom exhibits immediately after eating gluten and can persist for days. The feeling that it gives is confusion, trouble concentrating, and short term memory loss. A sufferer may forget to pick your children up from school, or even forget what they are writing mid sentence. Thankfully, this symptom does not persist as a person removes gluten from their diet. It may even make them feel finally awake after years of fogginess.
Recent studies have found that patients with Celiac disease commonly suffer from disordered sleeping, regardless of if the rest of their diet is healthy or not. Sleep disorders are more common to those suffering from Celiac disease vs. the rest of the general population. The disordered sleeping can be shown through an inability to fall asleep, and being unable to stay asleep. The study found that the causes of the inability to sleep well include depression, fatigue, and anxiety.
Many Celiac sufferers exhibit neuropathic symptoms. Problems with the neuropathic system can affect gross and fine motor control and sensory nerves. An undiagnosed Celiac disease sufferer my find their extremities exhibit nerve problems. This can include a tingling sensation in the hands and feet, ranging from mild to “fallen asleep”. Conversely, they may not feel anything in their hands and feet, as numbness is a common complaint. Other parts of the body may be affected, such as the facial muscles and body nerves.
Unfortunately, depression and suicide rates are higher in people with Celiac disease. Studies have found that even eating a gluten free diet, the rates of depression are much higher than the general population. One study found a connection between disordered eating and depression in women who suffer from celiac disease. As they closely monitor their foods for gluten, disordered and restrictive eating can develop. For suicide risk, it seems that once diagnosed and with dietary changes, the suicide risk is greatly reduced.

Almost anybody can tell you at least a little bit about gluten, as it has become quite the villain in today’s dietary world. In reality, gluten intolerance is a very serious issue and, although it may be up on the radar recently, it is more than just a passing fad.
Most people tend to consider gluten intolerance to be a food allergy or they may equate it with celiac disease. It is neither. It is a condition that occurs in the gut and if it is not cared for properly, it can affect your lifestyle in many ways.
When gluten proteins remain undigested in the gut, they are considered a foreign invader by the body and treated as such. As a result, your gut can become irritated and the absorption of food is reduced significantly.
Gastrointestinal issues can cause a number of uncomfortable problems, including pain, diarrhea and vomiting. When it comes to gluten intolerance, however, the signs may be similar or they could be quite different. Unfortunately, an issue with gluten intolerance often goes undiagnosed because most people continue to eat gluten and simply ignore the symptoms they are experiencing. Doing so can lead to additional diseases and autoimmune problems that could last a lifetime.
The following are 8 common signs that could point to gluten intolerance. If you are experiencing these symptoms with any severity, your doctor should be consulted.
1. Stomach Pain – One of the most common signs of gluten intolerance is stomach pain, along with other gastrointestinal issues. Those issues can include bloating, diarrhea, gas and constipation. When you eat foods that contain gluten, it can irritate the lining of the small intestine and can affect your ability to absorb vitamins and minerals from the food you’re eating.
2. Dizziness – Although most people would ignore this issue or consider it to be something else, gluten intolerance can often lead to disorientation, brain fog and feeling as if you are off-balance. Those issues are more likely to occur after you eat foods that contain gluten.
If you constantly have a cloudy feeling, don’t consider it to be normal, it isn’t! After you removed gluten from your diet, you may feel as if the cloud has been lifted from your thoughts.
3. Mood Swings – It is true that many different issues could lead to mood swings but gluten intolerance is one of those issues that should not be ignored. Many people that have such an intolerance feel as if they are anxious, irritable and upset for no reason after eating gluten.
4. Migraines – headaches can occur for many reasons as well but gluten intolerance can lead to chronic migraines and it should be considered a warning sign. Typically, the migraine will occur anywhere from 30 to 60 minutes after you eat.
5. Skin Itchiness – Due to the fact that your gut is having a problem processing gluten, inflammation is likely to follow. Your skin may also experience problems as a result of the inflammation, and it can show in a number of different ways. When your gut is unhappy, it can lead to dry, itchy skin and issues such as psoriasis and eczema.
6. Fibromyalgia – Approximately 4% of the population in the United States, mostly women, suffer from fibromyalgia. There are some rheumatology experts who feel as if gluten sensitivity may have a lot to do with the prevalence of fibromyalgia. It may not be directly related to it, but the gluten sensitivity could cause health problems that would lead to a secondary form of fibromyalgia.
7. Chronic Fatigue – When there are problems in the body, you are likely to feel mentally and physically exhausted. Even though you may be getting plenty of sleep at night, you still wake up in the morning feeling as if you are drained. This also has a lot to do with inflammation and the energy your body is expanding while it tries to manage the gluten proteins that you should not be eating.
8. Lactose Intolerance – The symptoms of gluten intolerance and lactose intolerance are very similar to each other. That is why it shouldn’t be surprising that individuals who have a problem with lactose may be more likely to have a problem with gluten proteins. In addition, dairy can lead to acid reflux and in turn, that can be a large part of gluten intolerance.
http://s-media-cache-ak0.pinimg.com/736x/fb/ab/ba/fbabbaa257a675ad0e98b7a766a477ba.jpg

http://41.media.tumblr.com/14560804980b1818a3561aeda763ef69/tumblr_ngzabat7Lc1tytybwo1_500.jpg
1. Freeze Yogurt in an ice cube tray
2. Put 1 1/4 cup of your favorite fruits in freezer bags
3. Add two frozen yogurt cubes in each fruit bag. Blend fruit mixture with 1 cup liquid of choice!
#WeightLoss #Smoothie
http://36.media.tumblr.com/9a2fa0cfad540b80252c76cbb36c46fd/tumblr_nk5tkpVjJf1unp1u4o1_500.jpg
#WeightLoss

http://s-media-cache-ak0.pinimg.com/736x/e6/51/6c/e6516c19f63cc4329c7b5b2e510b8179.jpg

http://s-media-cache-ak0.pinimg.com/564x/ec/38/35/ec3835c1162117e251e0f3e59e28bfb6.jpg

http://s-media-cache-ak0.pinimg.com/736x/7d/2c/52/7d2c521dc5e87b76771572394ed4c51d.jpg